


astigmatism,cornea,Cross-Linking,Eye Health,Featured,Keratoconus,Medical Technology
Corneal cross-linking is a treatment designed to help slow or stop the progression of a condition known as keratoconus. It does not replace glasses, contact lenses, or other vision correction options. Instead, its main goal is to strengthen and stabilize the cornea so the condition is less likely to continue worsening.
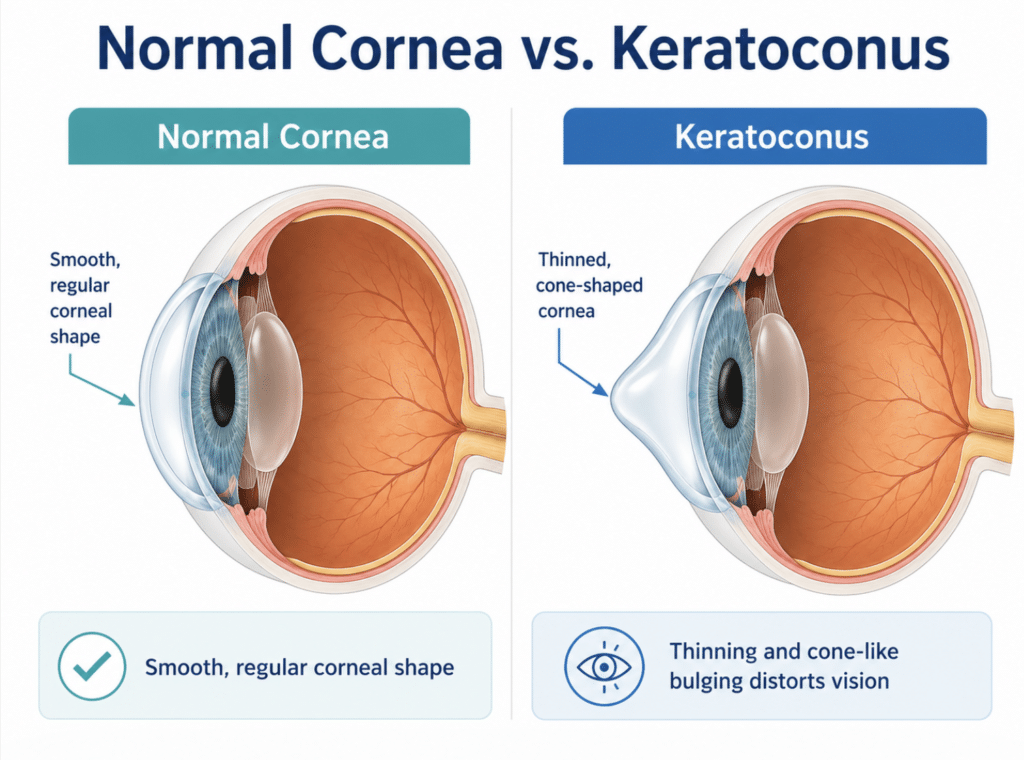
What Is Keratoconus?
Keratoconus is a progressive corneal condition where the normally round cornea becomes thinner and more cone-shaped. Since the cornea is responsible for focusing much of the light that enters the eye, even small changes in corneal shape can cause significant changes in vision.
Common symptoms of keratoconus may include:
- Blurry or distorted vision
- Increasing astigmatism
- Halos, glare, or starbursts around lights
- Difficulty with night driving
- Reduced vision even with updated glasses
Keratoconus often begins in the teenage years or early adulthood, although it can be diagnosed later. It may affect one eye more than the other, and progression can vary from person to person.
One of the most important goals in keratoconus care is early detection. The earlier progression is identified, the more opportunity there is to protect the cornea before the condition becomes more advanced.
How does Corneal Cross-Linking Work?
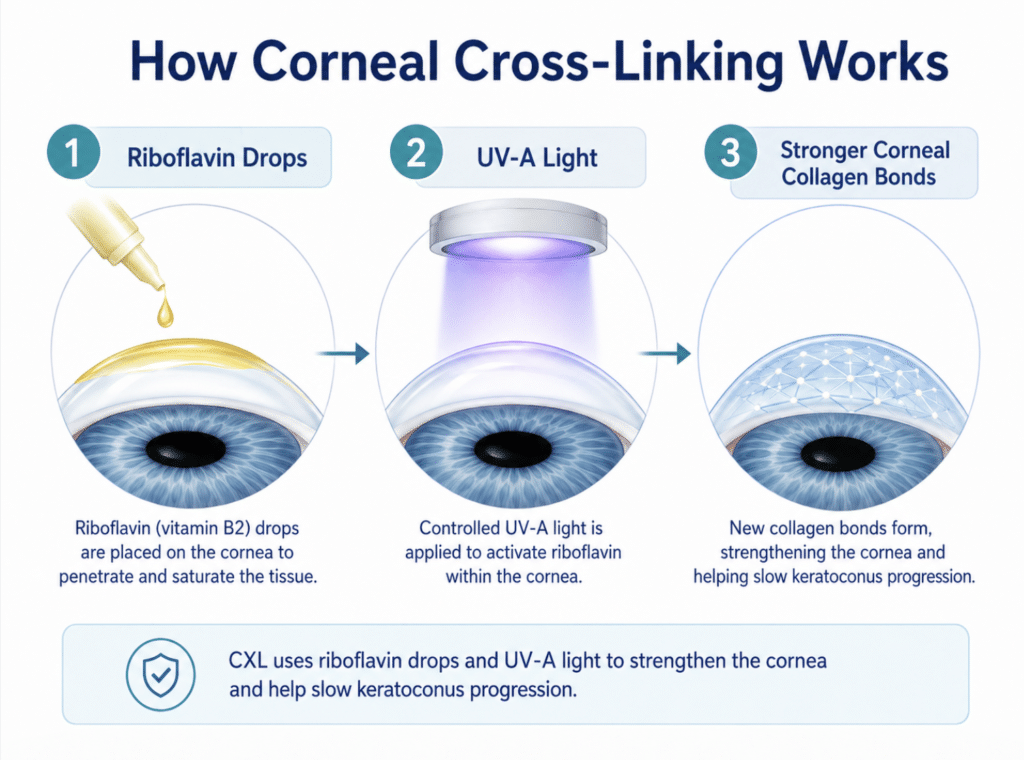
Corneal cross-linking is a minimally invasive treatment that uses riboflavin, also known as vitamin B2, and controlled ultraviolet-A light to strengthen the collagen fibers within the cornea.
Think of the cornea like a clear, flexible dome. In keratoconus, that dome becomes structurally weaker and begins to change shape. Cross-linking helps create additional bonds between the corneal collagen fibers, making the cornea more rigid and resistant to further bulging.
The main goal of CXL is not to “cure” keratoconus or fully reverse the corneal shape. The goal is stabilization.
For many patients, that is a very meaningful goal. Stabilizing keratoconus can help preserve vision, reduce the risk of further progression, and potentially reduce the future need for more invasive procedures such as corneal transplantation.
What Happens During Corneal Cross-Linking?
The exact protocol may vary depending on the patient and surgeon, but corneal cross-linking generally involves several key steps:
Who May Need Corneal Cross-Linking?
Corneal cross-linking is most commonly recommended for patients with progressive keratoconus or other forms of corneal ectasia.
A patient may be considered for CXL if testing shows signs such as:
- Increasing steepness of the cornea
- Progressive thinning of the cornea
- Increasing irregular astigmatism
- Changes on corneal topography or tomography
Not every patient with keratoconus needs immediate cross-linking. Some patients have stable disease and can be monitored closely. Others may show signs of progression and benefit from earlier intervention.
This is why proper diagnostic imaging is so important. Keratoconus cannot be fully assessed by prescription alone. Corneal mapping allows your eye care team to evaluate the shape, thickness, and stability of the cornea over time.
CXL and T-CAT: Stabilizing and Improving Corneal Shape
At North Toronto Eye Care, some patients with keratoconus may be candidates for a combined approach using corneal cross-linking and topography-guided custom ablation treatment, known as T-CAT.
CXL helps stabilize the cornea. T-CAT is designed to improve the corneal shape by reducing irregular astigmatism and higher-order aberrations. In selected patients, combining these approaches may help improve the quality of vision, reduce glare or ghosting, and make glasses or specialty contact lenses work better.
This combined approach is not appropriate for everyone. It requires careful assessment and a detailed discussion of risks, benefits, and expectations.
Frequently Asked Questions About Corneal Cross-Linking
Book a Keratoconus Consultation
Corneal cross-linking has changed the way keratoconus is managed. Instead of waiting for the condition to worsen, we now have options that can help stabilize the cornea earlier and protect long-term vision.
At North Toronto Eye Care, our team provides advanced diagnostic testing and personalized keratoconus treatment planning, including corneal cross-linking.
If you have been diagnosed with keratoconus or have been told you may have an irregular cornea, a detailed corneal assessment can help determine your next step. Call North Toronto Eye Care or request an appointment to learn whether corneal cross-linking may be right for you.
References:
- American Academy of Ophthalmology. Corneal Cross-Linking.
- Vohra V, Tadi P. Collagen Cross Linking for Keratoconus. StatPearls / NCBI Bookshelf.
- Cortina MS, Greiner MA, Kuo AN, et al. Safety and Efficacy of Epithelium-Off Corneal Collagen Cross-Linking for the Treatment of Corneal Ectasia. Ophthalmology. 2024.
- Larkin DFP, Chowdhury K, Burr JM, et al. Effect of Corneal Cross-linking versus Standard Care on Keratoconus Progression in Young Patients: The KERALINK Randomized Controlled Trial. Ophthalmology. 2021.
- Wollensak G, Spoerl E, Seiler T. Riboflavin/Ultraviolet-A-Induced Collagen Crosslinking for the Treatment of Keratoconus. American Journal of Ophthalmology. 2003.